Why the Flying Right Elbow Is Usually Not an Elbow Problem
The flying right elbow is one of the most commonly criticised positions in the golf swing, yet it is also one of the most misunderstood. It is easy to see on camera. It is easy to point at. It is easy to blame. But visible does not mean primary. In many golfers, the right elbow is not the original cause of the problem. It is the body’s visible compensation for a restriction that exists elsewhere.
When the body cannot create enough backswing depth through the ribcage, thoracic spine, scapula and shoulder complex, the arms are forced to continue the movement independently. The golfer still intends to complete the backswing. The club still has to travel to the top. The brain still expects a full position. But if the ribcage has stopped rotating and the lead-side tissues have reached their limit, the extra movement has to come from somewhere else.
This is why elbow-focused drills often fail. A golfer may place a towel under the right arm, rehearse a more connected position, or consciously force the elbow down, but the same pattern keeps returning. The reason is simple. The body still needs the compensation. Until the restriction that created the compensation is identified, the elbow will keep searching for the missing range.
Where the Golfer Should Look First
The golfer should not begin by looking only at the right elbow. The more useful starting point is to investigate where the body feels blocked during the backswing. In many cases, the most important locations are the left scapular border, the left lat, and the deep posterior shoulder tissue around the left and right deltoid region.
These areas matter because they are often where the restriction is felt before the elbow compensates. The golfer may feel a dense or blocked sensation beside the left shoulder blade. They may feel a stretch or grab beneath the left armpit or down the left side of the back. They may feel a deep restriction inside the back of the shoulder, as though the arm has reached its end point before the body has completed its turn.
These sensations are not irrelevant. They are often diagnostic clues. The body usually tells the golfer where movement is being blocked, but the golfer has often been trained to judge only what the swing looks like. The better question is not simply, “Where is the elbow?” The better question is, “Where does the body stop allowing the backswing to continue?”
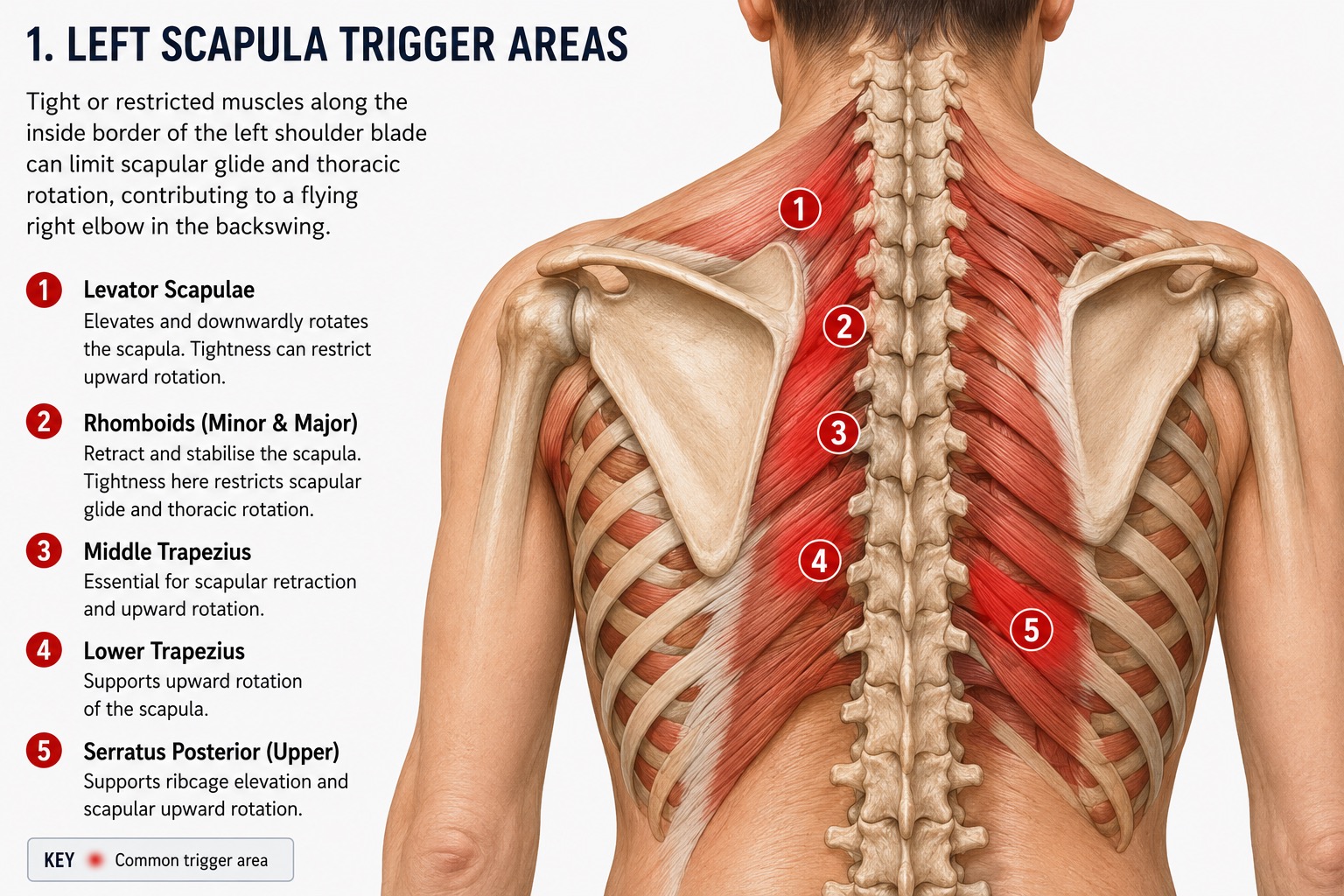
The Left Scapula Restriction
The left scapula plays a major role in the backswing. It must move across the ribcage as the body rotates. It cannot simply remain fixed. If the left scapula becomes restricted, the shoulder complex loses freedom, the ribcage loses rotational expression, and the golfer begins to run out of usable backswing depth.
The key area many golfers feel is along the inside border of the left shoulder blade. This region may involve the rhomboids, middle trapezius, levator scapulae, posterior cuff tissue and the surrounding fascial connections between the scapula and ribcage. If this region is stiff, overactive or protective, the scapula may not glide cleanly during the backswing.
When the left scapula cannot move efficiently, the body reaches a rotational limit earlier than it should. The golfer still tries to complete the backswing, so the arms continue moving. The right elbow then separates, not because it is the original fault, but because the torso and scapular system have stopped contributing enough movement.
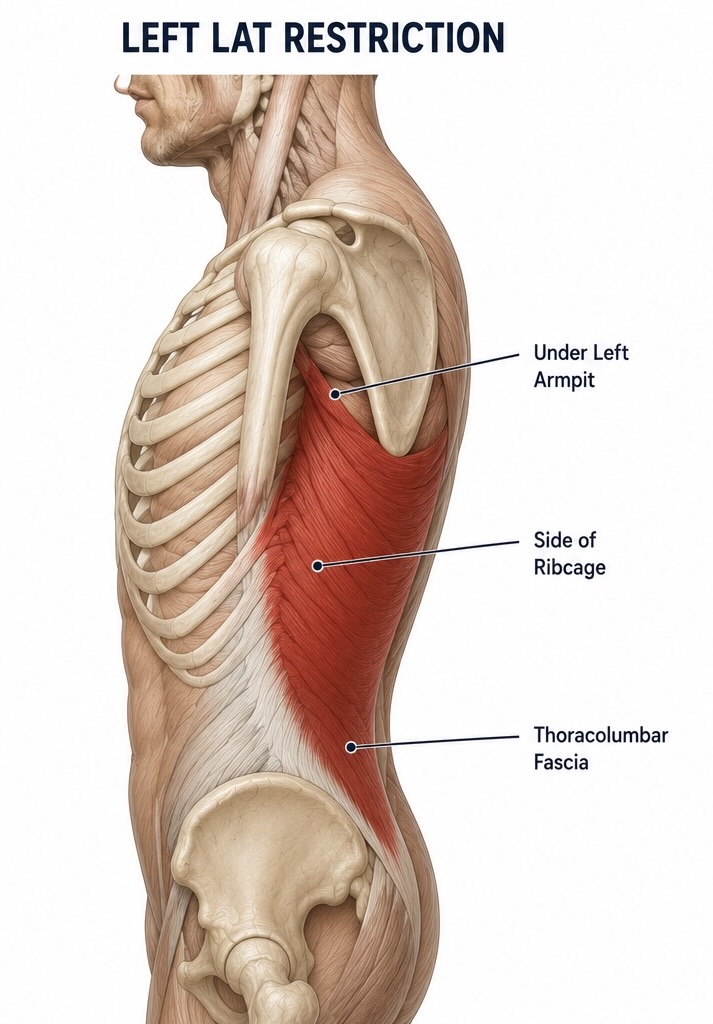
The Left Lat Restriction
The left lat is another key location. The lat is not a small isolated muscle. It is a large connection between the upper arm, trunk, pelvis and thoracolumbar fascia. In the backswing, the lead side must tolerate lengthening, rotation and elevation. If the left lat is tight or protective, it can block the ability of the lead arm, scapula and ribcage to organise properly at the top.
The golfer may feel this restriction beneath the left armpit, down the outer border of the shoulder blade, or through the side of the back. It may feel like the backswing reaches a hard end point. At that moment, the body has a choice. It can stop, or the arms can continue. Most golfers continue, which means the arms begin travelling without sufficient body rotation beneath them.
This is why the golfer should pay close attention to the felt location of the restriction. If the left lat becomes the area that limits the backswing, then right elbow correction alone will not solve the issue. The elbow is merely adapting to a left-side limitation.
The Posterior Shoulder and Deltoid Region
The posterior shoulder and deltoid region also need to be investigated. This applies to both shoulders, although the lead side often plays a major role in limiting backswing range. The golfer may feel a deep restriction around the back of the shoulder, inside the deltoid region, or around the posterior cuff. This may not feel like a simple stretch. It may feel like the shoulder joint itself has no more room.
This area is especially important because golf does not ask the shoulder to move in isolation. The shoulder has to move while the golfer is bent forward, holding a club, rotating the ribcage, controlling posture and organising the scapula. A shoulder may look acceptable in a basic clinical test, yet become restricted when placed into a golf-specific position.
| Area to Check | Common Sensation | Possible Swing Compensation |
|---|---|---|
| Left scapular border | Blocked, dense, tight or pinched beside the left shoulder blade. | The ribcage stops turning and the arms continue independently. |
| Left lat | Pulling beneath the left armpit or down the left side of the back. | The lead side cannot lengthen, so the trail elbow separates to find range. |
| Posterior shoulder | Deep restriction inside the back of the shoulder or deltoid region. | The arm path narrows and the right elbow moves outward. |
| Ribcage and thoracic spine | Turn feels complete too early, even though the backswing feels unfinished. | The arms take over and the elbow flies as a continuation strategy. |
Why Ribcage Rotation Changes the Right Elbow
Many golfers believe they have a shoulder turn problem when they actually have a ribcage rotation problem. The shoulders do not create the whole backswing by themselves. A significant amount of what is seen as shoulder turn comes from thoracic rotation and ribcage movement beneath the shoulders.
When the ribcage stops rotating, the arms are often dragged into a compensatory pattern. The hands continue travelling, the trail arm folds, and the right elbow begins to point outward. In this situation, the elbow is continuing a turn that the body could not complete.
This is why a golfer can repeatedly make the same elbow mistake, even when they understand the correct technical position. The nervous system is not making a random error. It is solving a movement problem. If the body cannot rotate enough, the arms continue the movement, and the elbow becomes the visible sign of that compensation.
Why Treatment on a Table Can Miss the Golf Problem
Traditional physiotherapy, massage, and soft-tissue treatment can be valuable, but a limitation is that much of it occurs with the golfer lying on a treatment table. In that position, the spine is supported, the shoulders are unloaded, the ribcage is relaxed, and the nervous system is operating in a completely different state from the golf swing.
The golf swing does not occur lying down. It occurs standing, bent forward, weight-bearing, gripping a club and rotating under load. A tissue that appears mobile or treatable in a passive position may become restrictive when the golfer assumes posture and attempts rotation. This is why a golfer can feel better after treatment but still reproduce the same flying elbow pattern when returning to the club.
Why Position-Specific Release Can Be More Relevant
A more golf-specific approach is to investigate the left scapula, left lat and posterior shoulder while the golfer is placed into controlled static backswing positions. This does not mean swinging at speed while someone applies pressure. It means placing the body into a safe static golf position where the restriction can be felt, then applying careful pressure to the relevant area.
A partner, coach, therapist or trained assistant may use a golf ball or massage ball to apply targeted pressure into the felt restriction while the golfer holds a static backswing position. The purpose is not to cause pain or aggressively force the tissue. The purpose is to explore whether the restriction changes when the area is contacted in the position where the problem actually appears.
This approach can be more relevant because the tissue is being assessed in the same context in which the restriction occurs. The spine is inclined. The ribcage is rotated. The scapula is loaded against the ribcage. The arms are positioned in a backswing shape. The nervous system is no longer experiencing the tissue in a passive state.
Practical Self-Assessment
The golfer can begin with a simple assessment. Move slowly into the backswing and notice where the body first says no. Do not judge the right elbow first. Feel the restriction first. Does the block appear beside the left shoulder blade? Does it appear beneath the left armpit? Does the left lat feel as though it stops the turn? Does the shoulder feel blocked deep inside the posterior deltoid region? Does the ribcage feel unable to continue rotating?
Then repeat the movement with careful manual pressure into the area, ideally with someone qualified or experienced enough to do this safely. If the backswing feels freer, if the elbow naturally organises better, or if the body can rotate without the same compensatory arm lift, the golfer has found a more meaningful source than the elbow itself.
Related Articles on Chris Brook Golf
This article connects closely to Why Golf Swing Changes Fail and How to Build Lasting Change, because both articles address the difference between visible technical faults and the deeper movement system that produces them.
It also connects to 3D Golf Biomechanical Analysis, because shoulder motion, thoracic rotation, scapular movement and pelvis control should be assessed together rather than treated as isolated body parts.
For a broader coaching framework, read Golf Coaching Services and Quiet the Mind, Lower the Score. These pages explain how technical movement, perception, psychology and performance behaviour must be understood as one integrated system.
Final Conclusion
The flying right elbow is often treated as a technical flaw, but in many golfers, it is a biomechanical message. The body is revealing that it cannot find enough movement through the rib cage, left scapula, left lat, or the posterior shoulder complex. When those structures reach their limit, the arms continue the backswing independently, and the right elbow flies.
The golfer should therefore investigate the key muscle locations that are felt during the backswing. The left scapular border, left lat and deep shoulder tissue are often more important than the elbow itself. If these areas restrict movement, the elbow becomes the compensatory joint.
The solution is not simply to force the right elbow down. The solution is to restore the movement that the elbow is compensating for. That requires assessing the body in the positions where the restriction actually appears. The golf swing happens in posture, under load and through rotation. Therefore, the most relevant intervention is often one that respects those exact demands.